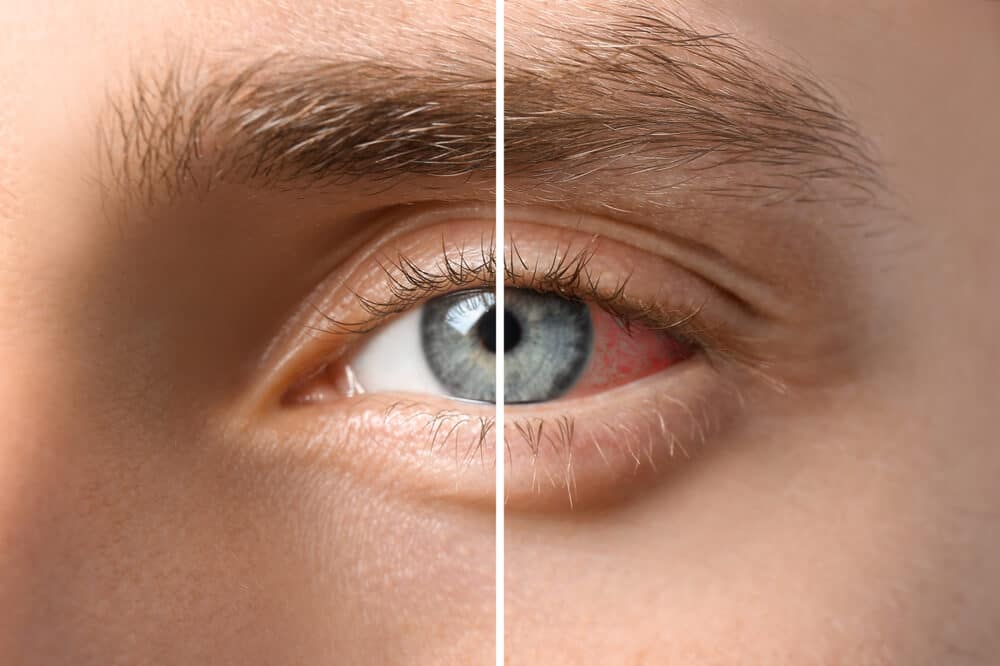
Uveitis refers to inflammation of the uveal tract, the middle vascular layers of the eye which are critical to its normal function. Because of the rich circulation of blood throughout this area and its proximity to other important parts of the eye, the uvea is susceptible to immune disorders which interfere with normal function.
Although many forms of uveitis are easily treated, some forms can be chronic and vision threatening. Uveitis is the fourth leading cause of blindness in the United States and, because of a wide variety of symptoms, it is most commonly diagnosed and treated by ophthalmologists.
Careful evaluation and management of uveitis is important to assure the best possible outcome for the patient. Uveitis occurs in all age groups, from young children to adults, and the age of onset helps define the type of inflammation
Various parts of the eye become swollen or inflamed due to uveitis and these fall into three broad categories: those in the front, middle and back of the uvea. The suffix “-itis” is used to describe inflammation due to disease so the following terms apply to specific parts of the eye when they are inflamed:
Symptoms of uveitis widely vary depending on the location of inflammation, rapidity of onset and the stage of the disease. Acute uveitis refers to a single episode of the disease while the term chronic uveitis refers to an ongoing disease condition. Patients with acute iritis will commonly be able to describe the specific onset of pain, sometimes giving the precise hour when symptoms first occur, as well as eye redness and excessive sensitivity to light. These symptoms are very easy for the patient with recurrent acute iritis to identify.
This is in contrast to the patient with intermediate uveitis or posterior uveitis, who may only complain of a poorly defined onset of increased floaters with an accompanying loss of central vision. Many of these patients have little or no pain or intolerance to light. Children who suffer from juvenile rheumatoid arthritis (JRA/JIA) may have ocular inflammation without any other symptoms.
Ophthalmologists who specialize in uveitis can diagnose many common clinical signs of uveitis which a patient may, or may not, be aware of experiencing. Treatment involves careful clinical evaluation and precise medication for the patient’s individual condition. Treatment goals always are to decrease inflammation and reestablish normality in the eye as quickly as possible. In many cases of chronic uveitis, it may not be possible to eradicate all of the intra ocular inflammation. Common secondary effects of uveitis include development of cataracts, glaucoma and macular swelling associated with macular scarring.
For many years the most successful treatments for uveitis have been eye drops, injections or the use of oral corticosteroids. In addition, dilating drops are often used to decrease ocular pain and prevent unwanted intraocular scarring.
Recently, new immune modulating agents have been developed which add to the successful treatment of uveitis. These more targeted drug solutions are seeing more widespread use. In addition, new drug delivery methods are being used for chronic uveitis conditions. Especially in patients with chronic inflammation, efforts are made to use steroid-sparing agents to minimize potential long-term systemic side effects of steroids. The side effects commonly experienced with each treatment used are always weighed against the potential benefits achieved through the treatment.
Most cases of acute iritis are initially treated with topical steroids or a combination of topical steroids and oral steroid supplement. Patients are advised that the most common form of acute iritis may last for 6 to 8 weeks, with possible recurrences.
Those patients with the more chronic uveitis may have a prolonged course of treatment, which never completely resolves the condition. In this situation, patients may experience significant vision impairment from macular edema (swelling), cataract or glaucoma.
It is important to maintain regular follow-up by your treating ophthalmologist in order to monitor medications as well as progression of the disease. Because of the serious complications which may occur as a result of uveitis, an ongoing partnership between patient and ophthalmologist greatly increases long-term success.
Wheaton Eye Clinic’s unparalleled commitment to excellence is evident in our continued growth. Today we provide world-class medical and surgical care to patients in six suburban locations—Wheaton, Naperville, Hinsdale, Plainfield, St. Charles, and Bartlett.
(630) 668-8250 (800) 637-1054